Research Study: Community Based Mental Health Training and Education for Local Public Service Organization Resiliency
The purpose of this project is to discover alternative means of improving mental health outcomes for local government in non-urban settings.
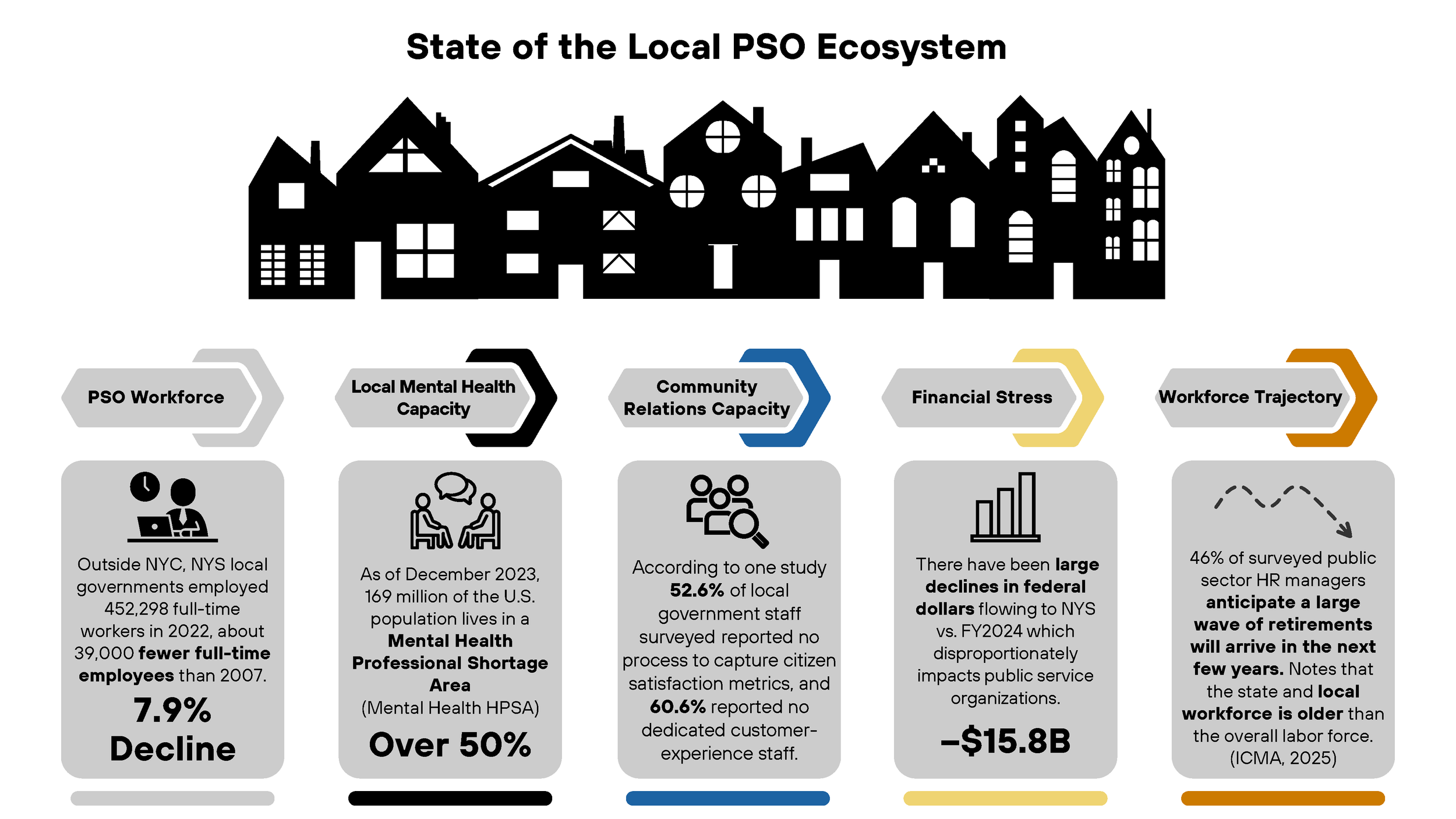
There is a broad understanding that many areas across NYS lack adequate behavioral health service providers and clinicians.
Local government organizations located in non-urban settings have more resource constraints that limit their ability to provide employees with access to mental health services.
Many mental health and behavioral health programs are not adapted for the unique pressures and stressors faced by local governments, most local government jobs outside of first responder roles, and rural cultural settings.
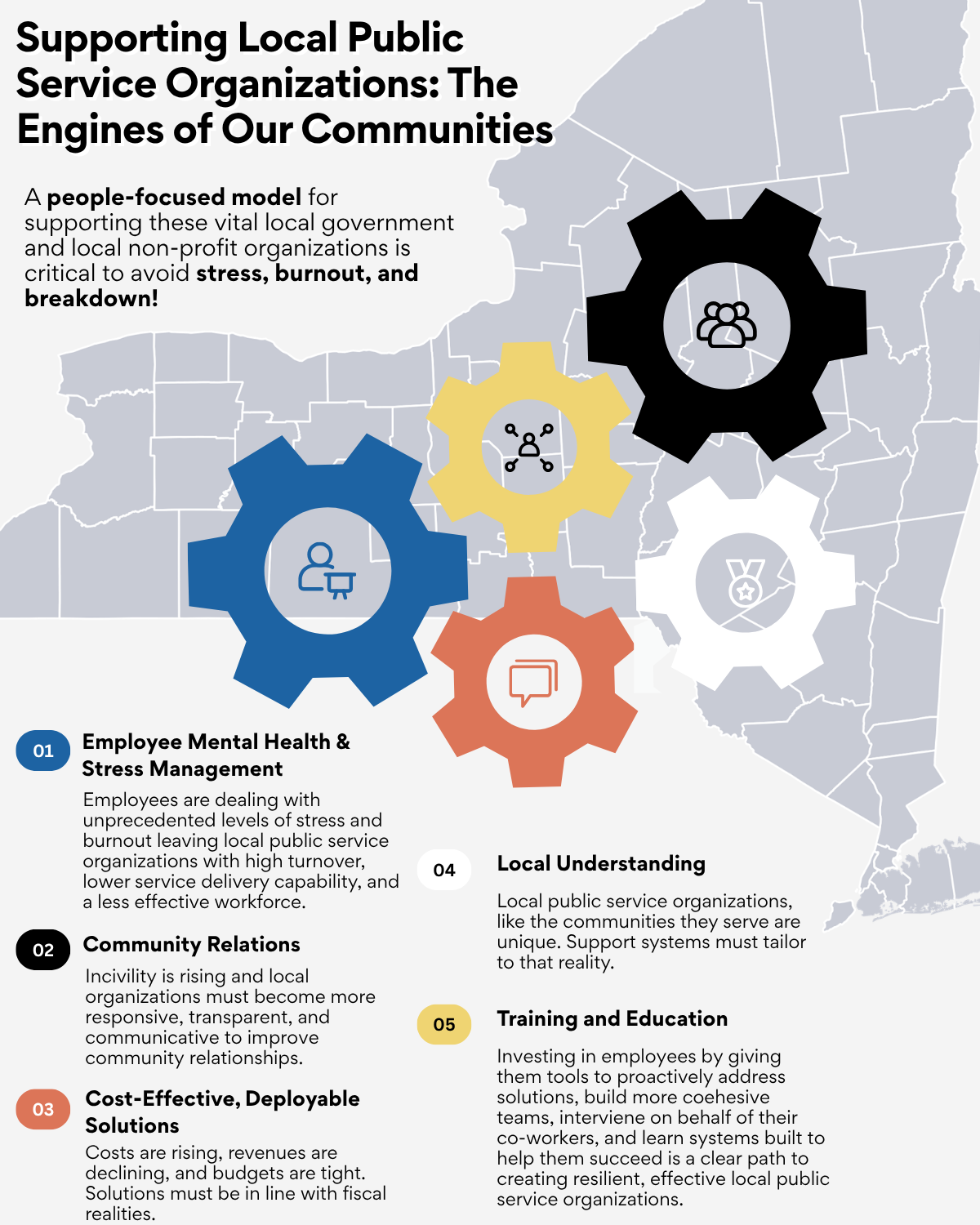
By collecting data about the mental/behavioral health needs of local government employees in non-urban areas, alternative methodologies for providing accessible, community-based, culturally adapted training can be proposed. The goal is to provide staff with evidence-based, non-clinical training, education, and support structures that create better long-term outcomes and more resilient local government organizations.
Gaps in Current Research:
A major gap is population and setting specificity. Much of the workforce mental health and burnout literature is centered on clinical/behavioral health providers, educators, or first responders. This proposal highlights a distinct group that is understudied: local government employees in non-urban settings, including roles that are not traditionally framed as “high-risk” but still face chronic stress related to public-facing demands, limited resources, and constrained access to services. The research lacks evidence on how these dynamics play out in small-town, county, village, or township environments where staffing is low and cultural nuances can create greater levels of stigma, confidentiality concerns, and impact help-seeking behavior.
A second gap is stressor relevance and measurement. This proposal focuses on pressures that are on the rise and directly impact local government work including public hostility/incivility, threats/harassment (including via social media), political/media scrutiny, regulatory/legal pressure, staffing/workload strain, and service-demand surges. These issues are not often measured together in existing studies, or they are often treated as generic “job stress.” That leaves uncertainty about which stressor categories are most strongly associated with burnout, turnover intent, and perceived effectiveness in this sector, and whether stressors differ meaningfully between public-facing and non-public-facing roles within local government organizations.
A third gap is what works outside of formal clinical services. Because many non-urban areas face provider shortages and access barriers, the most realistic near-term interventions are often non-clinical, community-based training and organizational support (e.g., de-escalation, mental health literacy, peer support norms, supervisor practices, debrief routines). Current research literature more commonly evaluates clinical access solutions (EAP availability, referral pathways, telehealth access).
Finally, there’s a gap in implementation and outcomes that matter to decision-makers. Even when trainings show promise, research in this space often underemphasizes the practical constraints this proposal elevates like backfill/coverage, scheduling lead time, budget ceilings, union/procurement/risk concerns. Current research often rarely connects these organizational constraints to sustainability and adoption in small organizations. Studies also frequently report individual-level wellbeing outcomes but less often link interventions to organizational outcomes (retention, absenteeism, service disruption, and service-quality proxies) or explain how change happens (e.g., via psychological safety, self-efficacy, stigma climate, supervisor support). This mixed-methods design explicitly addresses these “mechanism + feasibility + organizational impact” gaps.
Primary research question:
How are current political, economic, regulatory, staffing/workload, and service-demand pressures associated with stress, burnout, anxiety or depression among employees working in New York State local public service organizations, and to what extent can community-based mental health training and education lead to better organizational outcomes?